Diffuse cutaneous systemic sclerosis (dcSSc) is a progressive, severe systemic autoimmune disease which is characterised by inflammation and fibrosis of the connective tissue, leading to skin thickening, organ damage, limited daily functioning and premature death.
Unfortunately systemic sclerosis is incurable. However, there are treatments to stop or slow down disease progression by suppressing the immune system: cyclophosphamide (CYC), mycophenolate mofetil (MMF) or methotrexate (MTX), or resetting the immune system (stem cell transplantation).
Since 20 years, autologous stem cell transplantation (SCT) is used to treat systemic sclerosis. Two previous trials demonstrated that SCT was more effective compared to intravenous CYC with regard to skin and lung involvement and quality of life. However, SCT was also associated with a higher risk of severe, treatment-related complications. Because of the latter, SCT is mostly done in case other treatments fail.
On the other hand, upfront SCT, early in the course of the disease, could let to less complications and even be more effective, instead of later on in advanced disease.
Furthermore, when immunsuppressive medication does not work, severe organ damage due to disease progression could occur, leading to exclusion from SCT as a rescue treatment.
It is currently not known what the best treatment strategy in early dcSSc is, and what the optimal timing of SCT is.
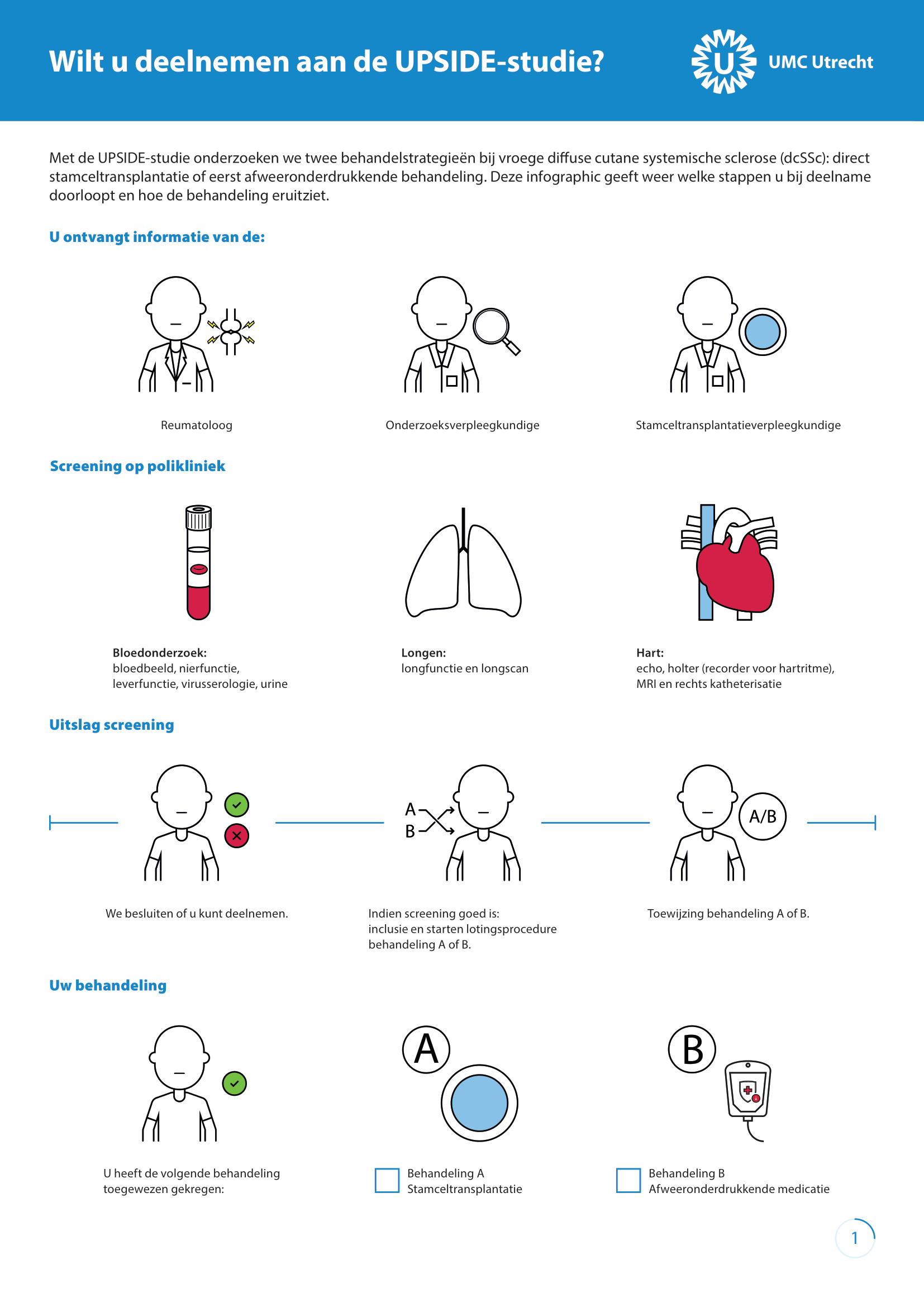
The UPSIDE trial investigates two treatment strategies in order to answer the question: Upfront SCT or SCT when other treatments fail?
Aan deze studie doen 7 centra in Europa mee. De toewijzing van behandeling vindt plaats door middel van loting (randomisatie), zowel patiënten als de behandeld arts en onderzoeker weet welke behandeling wordt gegeven (open label).
Adult patients with less then 3 years of disease duration and diffuse cutaneous skin disease with or without internal organ involvement can participate in this trial.
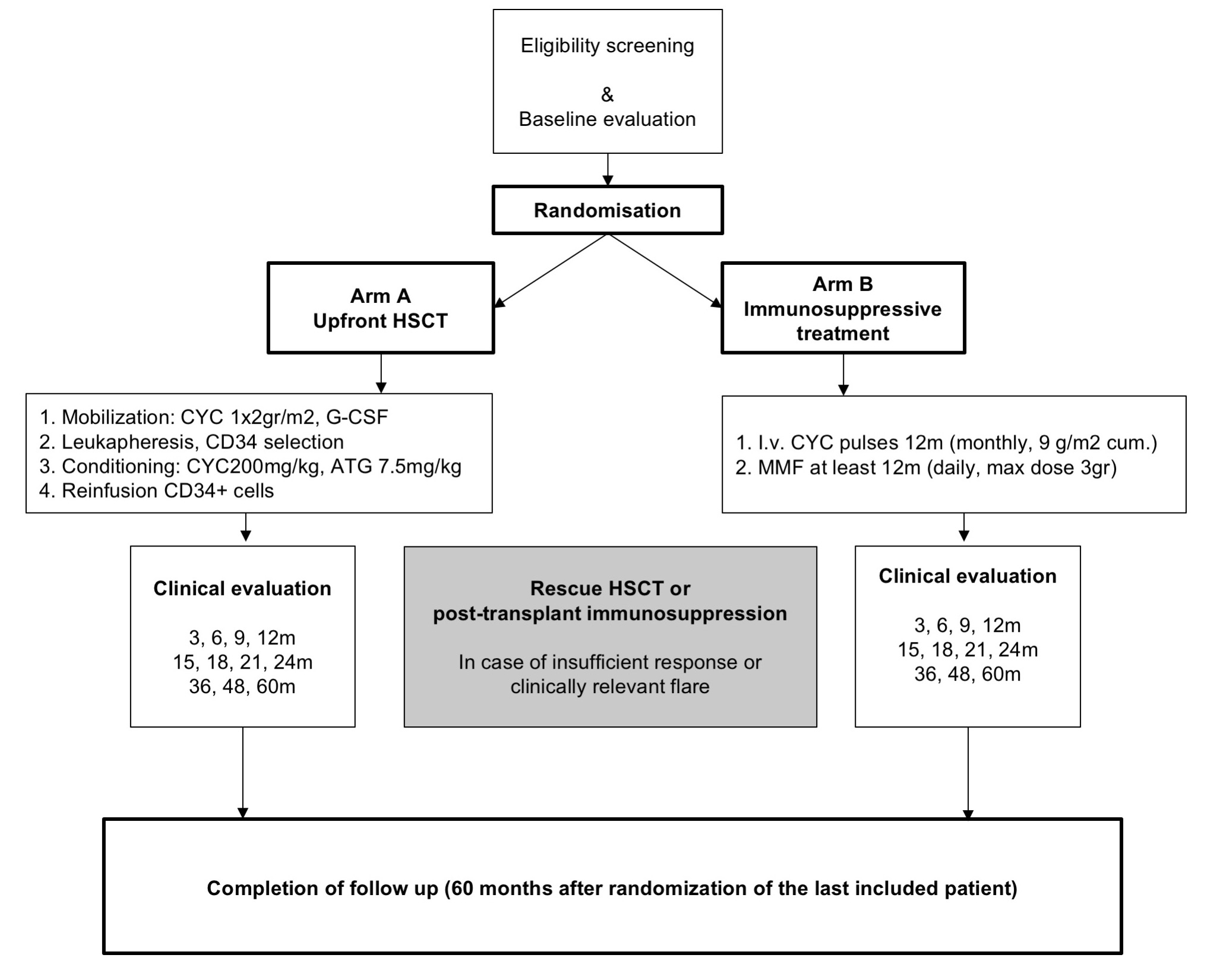
Patients will randomise for
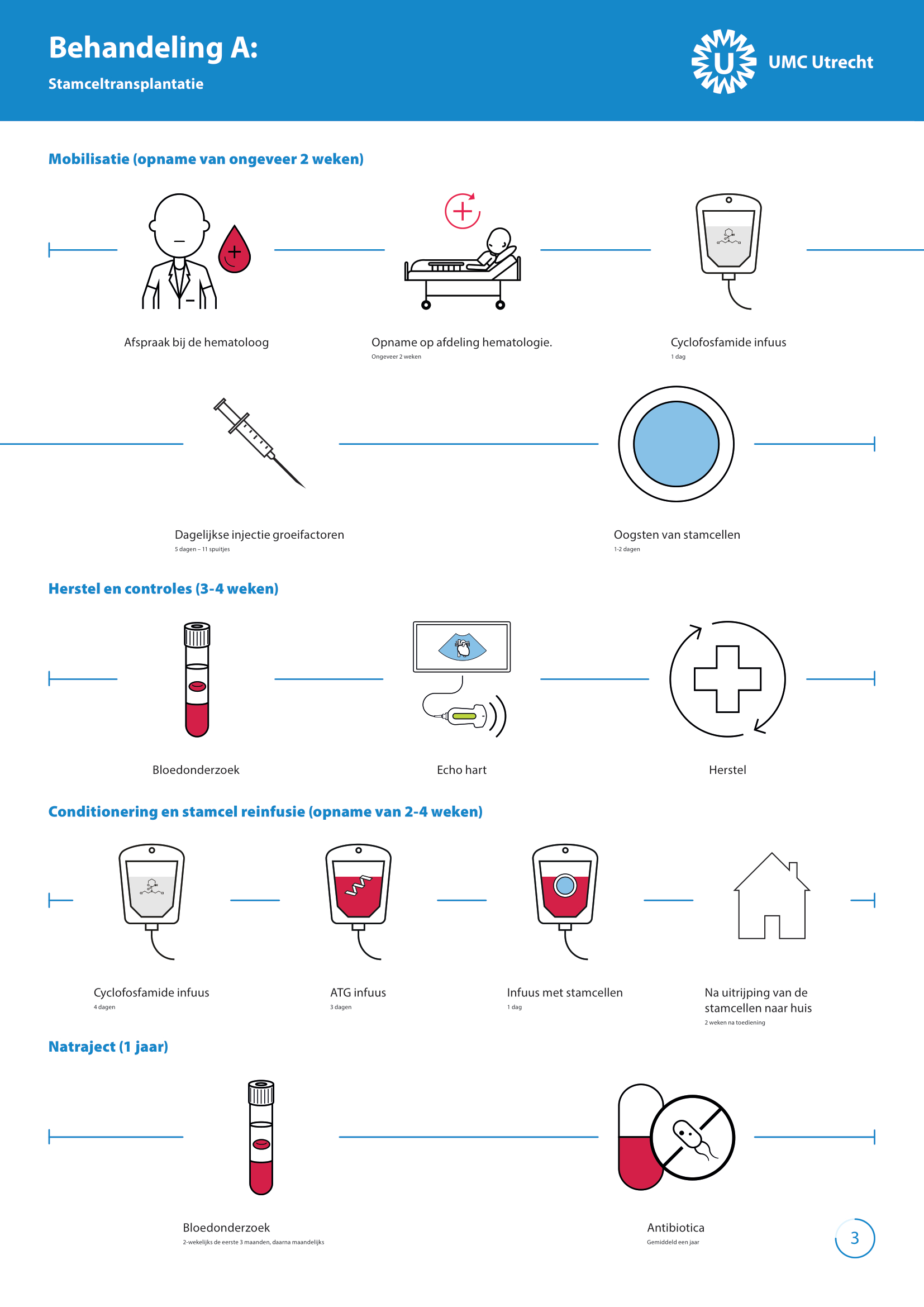
study arm A: upfront SCT or
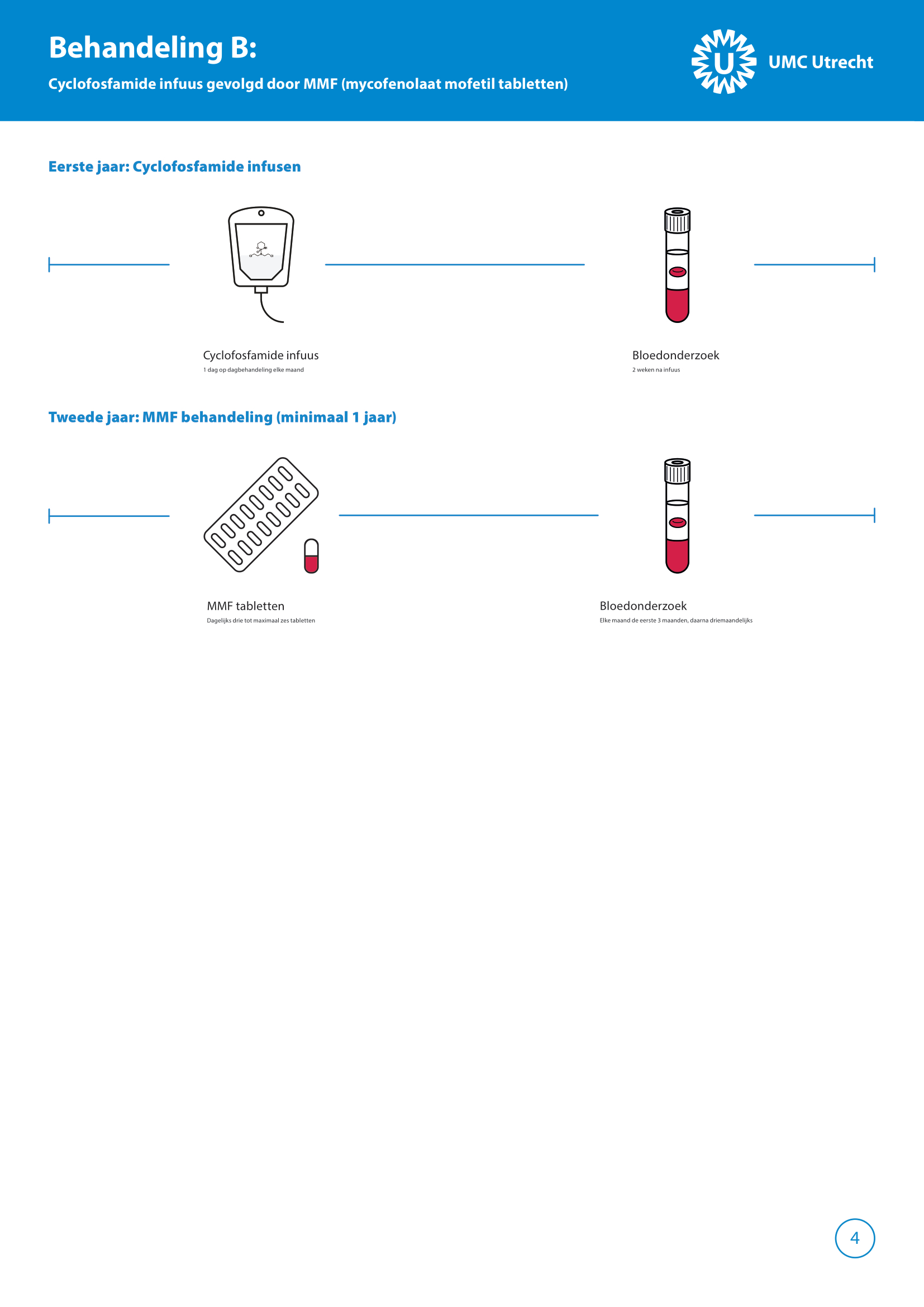
study arm B: immunosuppressive therapy first (1 year monthly iv cyclophosphamide followed by 1 year of MMF). If needed SCT can be provided in case of progression despite immunosuppressive therapies.
After completion of the trial we will compare outcomes in both study arms. Outcomes that will be evaluated are: progression free survival, changes in skin and lung involvement, treatment related complications, changes in microcirculation (nail fold capillaroscopy), changes in cardiac function, quality of life, daily functioning, sexual health, hand mobility, fatigue and work.
Results of this study will provide more insight in the optimal treatment strategy and will support patients and physicians in making treatment decisions.